Introduction
If you've ever felt a quiet, persistent sense of being too much or not enough — without knowing why — you're not imagining it. That feeling has a name, and it isn't a character flaw. It's one of trauma's most overlooked aftereffects: shame.
Not the fleeting embarrassment of a bad day. Something deeper. A background hum that colors how you see yourself, how you move through relationships, and whether you believe you deserve help at all.
This guide is written specifically for women carrying that weight — a compassionate, evidence-informed resource covering what trauma-related shame actually is, why women are disproportionately affected, how it shows up in daily life, and what healing looks like in practice.
Here's what you'll find:
- The difference between shame and guilt — and why it matters for recovery
- Reasons women face unique vulnerability to trauma-related shame
- The ways unaddressed shame affects mental and emotional health
- Evidence-based and holistic pathways to healing
- Simple practices you can start today
Key Takeaways
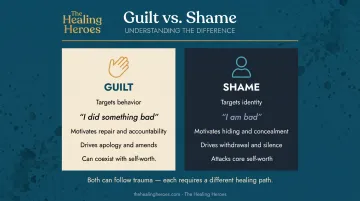
- Shame attacks your identity ("I am bad"), while guilt targets a behavior ("I did something bad") — each calls for a different healing approach
- Women face higher rates of interpersonal trauma, victim-blaming, and gender socialization patterns that make shame more deeply embedded
- Research across 3,663 participants found a significant moderate association between shame and PTSD symptom severity (r = .49)
- Shame is one of the biggest barriers to seeking help — naming it directly is already a step toward healing
- Recovery is possible through CPT, EMDR, Compassion-Focused Therapy, somatic practices, and narrative work
What Trauma-Related Shame Really Is (and How It Differs from Guilt)
Shame and guilt are often used interchangeably, but they operate very differently — and that difference matters for how you heal.
Guilt says: I did something wrong. Shame says: I am wrong.
Psychologist June Tangney's foundational research describes shame as a focus on the "bad self," while guilt focuses on "bad behavior." Guilt tends to motivate repair — apologies, accountability, making amends. Shame motivates hiding.
Chronic Shame Doesn't Feel Like Shame
Trauma-related shame isn't a momentary flush of embarrassment. It's a persistent internal state — a background sense of unworthiness, defectiveness, or defilement that can feel less like an emotion and more like a fact about who you are.
That's what makes it so hard to recognize. Chronic shame often becomes invisible, surfacing not as shame itself but as:
- Anxiety and hypervigilance
- Perfectionism ("if I'm good enough, no one will see how broken I am")
- Constant self-criticism
- A nagging sense of never being enough
This is sometimes called "bypassed shame" — shame that shows up as other emotional states, or gets masked through overachievement or withdrawal.
Shame and PTSD: Closer Than You Think
The DSM-5 formally recognizes shame under PTSD's Criterion D, which includes "persistent negative emotional state" and persistent negative beliefs such as "I am bad." Shame isn't just a side effect of PTSD — research increasingly views it as a core driver of PTSD symptoms.
Shame is self-reinforcing in a way most emotions aren't. Because shame is itself considered shameful, people hide it. That silence keeps them stuck — and it's precisely why naming it out loud, or even on the page, is already part of the work.
Why Women Are Particularly Vulnerable to Trauma-Related Shame
Women aren't more prone to shame because of something inherent. They're more exposed to the specific types of trauma most strongly linked to shame — and to cultural messages that amplify it.
The Exposure Reality
The data is stark:
- At least 1 in 4 girls experience child sexual abuse, compared to 1 in 20 boys
- 19.6% of women have experienced intimate partner contact sexual violence in their lifetime, versus 7.6% of men (CDC NISVS)
- Approximately 1 in 6 women have experienced attempted or completed rape, compared to 1 in 33 men
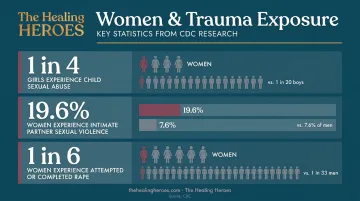
These aren't abstract statistics. Sexual violence, childhood abuse, intimate partner violence, and betrayal trauma are the categories of experience most strongly linked to shame — and women experience them at dramatically higher rates.
How Culture Embeds the Shame
Exposure alone doesn't explain everything. Cultural messaging does the rest.
Victim-blaming narratives — what were you wearing, why didn't you leave, why didn't you say something sooner — are external messages that become internalized, especially when encountered repeatedly or during childhood. Research by Catton et al. (2023) found that shame may be the affective mechanism through which invalidating judgments silence sexual violence survivors.
Gender socialization compounds this further. Many girls are raised to prioritize others' needs, suppress anger, and take responsibility for relational harmony. When trauma occurs, this conditioning often translates into what did I do wrong? rather than why did someone do this to me?
Mental Contamination: A Shame-Based Body Experience
For women who have experienced sexual violence specifically, there's mental contamination — a feeling of internal dirtiness without any physical contaminant. Research by Badour et al. (2013) describes it as a somatic shame experience that can persist for years and drive self-punishing behaviors.
It's not general guilt. It's shame that lives in the body.
That somatic experience becomes even harder to untangle when early childhood trauma is part of the picture. When neglect or abuse comes from caregivers, it creates deep shame-related internal templates that adult trauma can reactivate. For women who've experienced both, these layers compound — making it feel like evidence that they are fundamentally flawed.
How Trauma-Related Shame Shows Up in Daily Life
Most women carrying trauma-related shame don't identify it as shame. They identify it as anxiety, relationship problems, or just "how they are." These patterns are worth recognizing.
Behavioral Signs
Common shame-avoidance strategies that often go unrecognized:
- Difficulty saying no, constant over-apologizing
- Shrinking in relationships, difficulty receiving care or compliments
- Self-isolation after conflict or perceived failure
- Perfectionism as a way to "earn" worthiness
- Withdrawal from situations where there's any risk of judgment
Studies on complex PTSD (including work by Herman, 1992, and van der Kolk, 2014) consistently find that social withdrawal, concealment, and intimacy difficulties are linked to shame responses — not personality traits.
The Inner Critic
The self-talk of trauma-related shame is distinctive. It sounds like:
- "I'm too much for people."
- "If they really knew me, they'd leave."
- "I don't deserve good things."
- "I ruin everything I touch."
This isn't a personality flaw. It's a learned protective strategy — a voice that developed to make sense of what happened and keep you safe from further harm. Recognizing it as protection rather than truth is often the first shift that makes it possible to work with.
Shame in the Body
Shame doesn't just live in the mind — it shows up in the body. Research by Scheffers et al. (2017) found that women treated for early childhood trauma showed impaired body experience — including body awareness, body attitude, and body satisfaction — associated with both trauma severity and dissociation.
Disconnection from the body is one of shame's most common expressions. This is why healing approaches that work with the body, not just with thought patterns, are often so important for women.
The Mental Health Impact of Unaddressed Shame
Shame doesn't stay contained. Left unaddressed, it spreads — feeding depression, disconnection, and avoidance behaviors that compound over time.
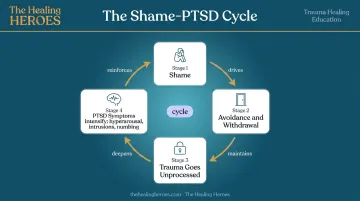
The Shame-PTSD Loop
A 2019 meta-analysis across 3,663 participants found a significant moderate association between shame and PTSD symptoms (r = .49). More recent research by McCann et al. (2023) found trauma-related shame prospectively predicted daily PTSD symptoms — even after accounting for guilt.
The mechanism is avoidance. Shame drives hiding and withdrawal, which prevents trauma from being processed. Unprocessed trauma then maintains and worsens PTSD symptoms — hyperarousal, intrusive thoughts, emotional numbing — which intensifies shame further. Each stage reinforces the next.
Coping Strategies That Deepen the Cycle
When shame-related distress becomes unbearable, people reach for whatever relieves it — and those strategies often create their own problems:
- Substance use: A systematic review of 27 studies found increased shame is associated with greater substance use among survivors of interpersonal violence
- Disordered eating: Sexual interpersonal trauma is associated with anorexia nervosa and binge-eating disorder, with shame identified as a key mechanism
- Emotional shutdown: Cutting off feeling entirely as a way to not feel this
These aren't character failures. They're attempts to manage pain that has nowhere else to go. The problem is they tend to generate more shame, tightening the cycle.
Why the Most Affected Women Often Reach Out Last
Shame creates the belief that you are unworthy of support — that disclosure will lead to judgment, that healing is something that happens for other people. Research confirms that avoidance of trauma disclosure mediates the link between trauma exposure and PTSD severity.
The women who most need help are often the least likely to reach for it. That's not a personal failing. That's shame functioning exactly as it's designed to — keeping you isolated from the very resources that interrupt it.
Pathways to Healing: Evidence-Based and Holistic Approaches
Healing from trauma-related shame doesn't follow a single path. Different approaches work at different levels — thought patterns, stored memory, the body, the story you tell yourself. What matters is finding what fits where you are right now.
Cognitive Approaches: Challenging Shame-Based Beliefs
Cognitive Processing Therapy (CPT) directly targets what researchers call "stuck points" — the internal beliefs that sustain shame. These typically follow a pattern: it was my fault, I am permanently broken, this defines everything about me.
A randomized controlled trial by Resick et al. (2002) of 171 female rape survivors found CPT effective for PTSD, with particularly strong reductions in guilt cognitions. CPT works by helping women move from "I deserved what happened" toward a more accurate understanding of the trauma and their role — or lack of role — in it.
EMDR: Working with How Shame Is Stored
EMDR (Eye Movement Desensitization and Reprocessing) is recommended by both the WHO and APA for PTSD treatment. What makes it particularly relevant for shame is that it works with how traumatic memories and shame-based self-beliefs are stored in the nervous system — not just in thought patterns.
Many women find it shifts core beliefs like "I am damaged" at a level that talk therapy alone doesn't always reach. EMDR commonly targets:
- Intrusive memories tied to the moment of trauma
- Body-level fear responses that persist despite conscious reframing
- Deep self-beliefs formed in the aftermath ("I am broken," "I brought this on myself")
- The emotional charge that keeps shame active long after the events themselves
The Healing Heroes podcast has featured expert conversations on EMDR — including an episode with licensed clinical social worker Jen Baumgold — for listeners wanting to explore this further.
Compassion-Focused Therapy and Shame Resilience
Compassion-Focused Therapy (CFT), developed by Paul Gilbert, directly targets the self-critical voice at the heart of shame. It helps build an internal relationship of safety — recognizing that the shame you carry is a learned response to overwhelming experiences, not a truth about who you are.
Brené Brown's Shame Resilience Theory offers an accessible framework alongside CFT:
- Recognize shame and understand its triggers
- Practice critical awareness of cultural and social messages that amplify it
- Reach out to someone you trust
- Speak shame — because shame loses power when named aloud

Somatic and Holistic Approaches
Because shame is embodied, body-based approaches are often essential, not an add-on. A randomized controlled trial by Brom et al. (2017) found Somatic Experiencing significantly reduced PTSD symptoms (Cohen's d = 1.26). Somatic Experiencing, mindfulness, breathwork, and movement-based practices work directly with the physical responses — tension, shutdown, hyperarousal — that cognitive work doesn't resolve on its own.
The Healing Heroes podcast explores many of these modalities through expert conversations — including episodes on myofascial release, yoga, breathwork, and somatic healing — for women still figuring out where to start.
Narrative and Expressive Writing
Narrative work helps externalize shame: the trauma happened TO you, it is not WHO you are. Written Exposure Therapy has been found as effective as Prolonged Exposure for PTSD symptom change, with less dropout.
Structured writing with self-compassion can help women reclaim their story from shame — one word at a time. Approaches include:
- Written Exposure Therapy — short, focused writing sessions returning to traumatic memories with guided structure
- Unsent letters — expressing what couldn't be said aloud to people or situations involved in the trauma
- Resilience journaling — deliberately documenting moments of strength to build a counter-narrative to shame
Simple Ways to Support Yourself (and Others) Today
Practices to Begin Now
These don't require a therapist or a major commitment. They work alongside whatever else you're doing:
Notice shame-based self-talk without judgment. When you hear the inner critic, try: "I'm having a shame response right now. This is a feeling, not a fact." That small reframe interrupts the automatic loop.
Build small moments of safe connection. Shame thrives in silence. You don't need to disclose everything — even one honest conversation with someone you trust shifts the dynamic.
Use grounding and breath to regulate shame flares. Slow, deliberate breathing activates the parasympathetic nervous system, creating a physiological counterweight to shame's hyperarousal. Five slow breaths, feet on the floor, name five things you can see.

If You're Supporting Someone You Love
- Listen without trying to fix. Presence matters more than solutions.
- Don't say "you have nothing to be ashamed of." It's well-intentioned, but it can inadvertently communicate that their feelings are wrong — which deepens shame.
- Avoid expressions of shock or disbelief, even unintentionally. Reactions that confirm the person's fear of being "too much" make disclosure feel more dangerous.
- Ask what they need rather than assuming.
The Case for Professional Support
Reaching out for help doesn't mean you're broken. It means you're directly countering shame's core lie: that you are unworthy of support.
A trauma-informed therapist can make a real difference, and finding the right fit is worth the effort. Different modalities work for different people, and trying more than one isn't a detour — it's just how healing tends to go.
Frequently Asked Questions
What is the difference between trauma-related shame and guilt?
Guilt relates to a specific behavior — "I did something wrong" — and often motivates repair. Shame is an attack on the entire self: "I am wrong, broken, or unworthy." Both can follow trauma, but they show up differently and require different healing approaches. CPT, for example, directly addresses the self-blaming cognitions that drive both.
Why do women often experience more trauma-related shame than men?
Women experience significantly higher rates of sexual violence, childhood sexual abuse, and intimate partner violence — the categories of trauma most strongly linked to shame. Victim-blaming cultural messaging and gender socialization patterns that encourage self-blame amplify and embed shame more deeply in women's self-concept.
Can trauma-related shame go away on its own without therapy?
Some people find meaningful relief through community, self-compassion practices, and safe relationships. But deep-rooted trauma shame is self-reinforcing by nature: it tends to intensify when left unaddressed rather than resolve on its own. Professional support typically makes a significant difference.
How does trauma-related shame affect relationships?
Shame creates fear of exposure and rejection, leading to withdrawal, difficulty trusting, people-pleasing, and emotional disconnection. Intimacy requires vulnerability, and shame makes that feel too dangerous — even in relationships where connection is genuinely available.
Is trauma-related shame the same as having PTSD?
They're related but not identical. Shame is recognized in the DSM-5 as part of PTSD's diagnostic criteria, and high shame levels are a strong predictor of PTSD severity. But shame can be present without a full PTSD diagnosis, and addressing shame directly is relevant whether or not PTSD is formally diagnosed.
What should I do if I recognize trauma-related shame in myself?
That recognition matters. It means you're already seeing what you're carrying more clearly. Start with self-compassion: name what you're experiencing without judgment, talk to one trusted person, and consider reaching out to a trauma-informed therapist. Shame heals in connection, not isolation.