Introduction
You're mid-conversation when it happens. Someone says something that should land — something important — and you just... go blank. You hear the words. You might even respond. But inside, there's nothing. No anger, no sadness, no relief. Just a kind of hollow quiet where a feeling should be.
That blank isn't weakness, and it isn't a choice. For many women, it's the nervous system doing exactly what it learned to do: protect you.
Emotional shutdown is a recognized trauma response — one that shows up in women in particular ways that rarely get named for what they are. According to CDC data, 27.2% of women experience coercive control and entrapment by an intimate partner in their lifetime. The nervous system keeps score of all of it.
Here, you'll find what shutdown actually is, why women are especially vulnerable, how to recognize it in yourself, and what healing can look like — including body-based and relational approaches built around how your nervous system actually works.
Key Takeaways
- Emotional shutdown is an involuntary nervous system response to threat — not a character flaw
- Women face disproportionate exposure to the relational trauma most linked to shutdown
- Shutdown doesn't resolve through insight alone; it requires new experiences of safety
- Body-based therapies, trauma-informed care, and safe connection are the core paths to healing
- Reaching out for support is how healing begins; your nervous system needs new experiences, not just willpower
What Is Trauma-Related Emotional Shutdown?
Emotional shutdown isn't simply feeling sad, tired, or checked out after a hard week. It's a specific physiological state — the nervous system's last-resort protective response when both fight and flight feel impossible.
The Three Nervous System States
Stephen Porges' Polyvagal Theory, introduced in 1995, maps three autonomic states that every human nervous system cycles through:
| State | Function | What It Feels Like |
|---|---|---|
| Ventral vagal (social engagement) | Safety, connection, flexible regulation | Calm, present, able to connect |
| Sympathetic (fight-or-flight) | Mobilized defense | Anxious, activated, urgent |
| Dorsal vagal (shutdown/collapse) | Defensive immobilization | Blank, frozen, disconnected |
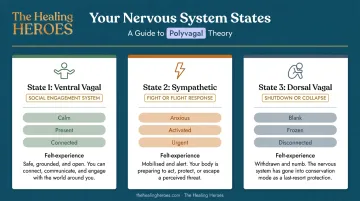
Shutdown is the oldest and most involuntary of the three. The broader defense-cascade research documents what happens physiologically during collapse: decreased heart rate, reduced respiration, impaired speech, blank facial expression, loss of muscle tone, and dissociation.
The mind goes offline. Thinking turns foggy, and memory becomes unreliable.
How Trauma Creates a Shutdown Pattern
Shutdown makes sense as a survival response. When the threat is overwhelming and escape isn't possible, the nervous system stops broadcasting — it goes quiet to survive.
The nervous system learns this pattern. Trauma memories and cues tied to the original threat can re-trigger shutdown long after the danger has passed — a raised voice, a dismissive tone, the particular pressure of a conversation that feels too close. The body responds before the mind has a chance to evaluate whether the threat is real.
The difference between occasional emotional numbness and chronic shutdown rooted in unresolved trauma is persistence and pattern. If you're regularly going blank, withdrawing, or feeling cut off from your own emotional experience, that pattern is worth paying attention to.
Why Women Are Particularly Vulnerable to Emotional Shutdown
Shutdown doesn't happen in a vacuum. Certain experiences make the nervous system far more likely to default to collapse, and women face a disproportionate concentration of them.
Relational Trauma and the Betrayal of Safety
The trauma most strongly linked to shutdown is relational trauma: threat that came from within a relationship. Abuse, assault, coercive control, neglect. When the person who should provide safety becomes the source of danger, the nervous system faces a particular bind — the social engagement system itself starts to feel like a threat.
In a study of 298 women following sexual assault, 70% reported significant tonic immobility during the assault, and 48% reported extreme tonic immobility — meaning shutdown was the most common involuntary response, not resistance. This matters for how survivors understand their own reactions.
Socialization, Dismissal, and Depletion
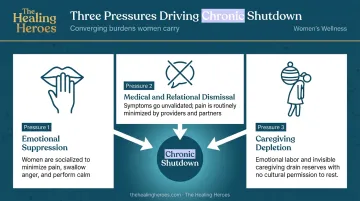
Three converging pressures push women toward chronic shutdown:
- Emotional suppression: Women are socialized to manage and minimize their emotional responses for others. That chronic pressure to "hold it together" creates nervous system strain that erodes regulation over time.
- Medical and relational dismissal: Research documents consistent gender bias in pain care — women's distress is frequently minimized or pathologized. When expressing pain repeatedly leads to being dismissed, the nervous system eventually stops broadcasting.
- Caregiving depletion: Women comprise approximately 60% of unpaid caregivers, according to long-term caregiving research. Caring for others while disconnecting from one's own inner experience is a functional form of shutdown: present on the outside, absent on the inside.
The Shame That Compounds It
The shame cycle adds another layer. Women in shutdown often blame themselves for it. I should feel more. Something is wrong with me. I'm broken.
That self-blame is itself part of the trauma pattern — and it deepens shutdown rather than resolving it.
Recognizing the Signs of Emotional Shutdown in Yourself
Shutdown can be subtle. It doesn't always look like crisis. Sometimes it looks like competence. Recognizing where it shows up — internally, relationally, and in your body — is the first step toward working with it rather than around it.
Internal Signs
- Feeling emotionally flat, blank, or disconnected from your own reactions
- Difficulty naming feelings when someone asks — not because you're avoiding the question, but because nothing comes
- A sense of watching your life from a distance, like an observer rather than a participant
- Loss of interest in things that once brought genuine pleasure
These internal experiences often ripple outward into how you show up with others.
Relational and Behavioral Signs
- Going quiet or blank during emotionally charged conversations
- A pull to leave the room or withdraw from closeness — not out of preference, but compulsion
- People-pleasing on autopilot with no felt emotional connection to any of it
- Difficulty trusting others even when the situation is genuinely safe
Somatic (Body-Based) Signs
The body often speaks what the mind can't name yet:
- Shallow, restricted breathing
- A collapsed or heavy posture
- Jaw tightness or clenching
- Heaviness or limpness in the limbs
- A sense that the body has become unfamiliar — disconnected or "not quite yours"
- A "pressure behind the eyes" quality, or a foggy, underwater feeling
These aren't imagined symptoms. Peer-reviewed research on tonic and collapsed immobility documents bradycardia, decreased respiration, immobility, and dissociation as physiological components of defensive collapse.
Why Emotional Shutdown Doesn't Simply Resolve on Its Own
Here's the part that often surprises people: understanding what shutdown is doesn't make it stop.
The nervous system learned shutdown as a survival strategy. Survival strategies don't switch off because you've read about them. They require new experiences of safety to actually rewire.
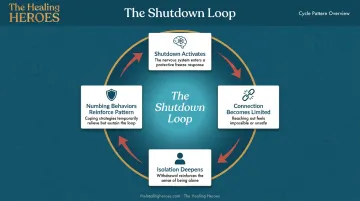
The Self-Reinforcing Cycle
Shutdown creates a painful catch-22:
- Shutdown limits connection with others
- Safe connection is precisely what brings the nervous system back online
- So the isolation, withdrawal, and numbing behaviors that feel protective — overworking, overeating, substance use — can deepen the pattern rather than relieve it
That loop has research behind it: substance use and PTSD symptoms can maintain each other through self-medication and ongoing avoidance, while experiential avoidance erodes the social support that most protects against trauma-related outcomes.
How Long Can Shutdown Last?
Duration varies considerably. Two clinical distinctions matter here:
- Acute Stress Disorder: symptoms appear within the first month after trauma exposure
- PTSD: symptoms persist beyond one month
For women who have experienced repeated or developmental trauma, shutdown can become a chronic baseline state — not a temporary reaction but a chronic background state.
Duration is one of the clearest signals for when to seek professional support. If shutdown has been your baseline for weeks or months, that pattern isn't going to shift on its own.
Healing from Emotional Shutdown: Approaches That Can Help
Healing from shutdown isn't about forcing yourself to feel. It's about creating the conditions where feeling becomes safe again.
Safety and Self-Compassion Come First
The nervous system needs evidence (not argument) that emotional expression won't lead to punishment, abandonment, or overwhelm. Environment and relationship matter as much as technique. Before any modality can work, some degree of safety has to exist.
Self-compassion isn't soft. For a nervous system conditioned to shut down in response to distress, receiving one's own pain with kindness is genuinely new information. That kindness is the first signal that something has changed.
Body-Based Approaches
Because shutdown lives in the body, healing often has to start there before words are possible.
Practical starting points:
- Notice physical sensations without trying to fix or change them — just attend to what's present
- Move slowly and intentionally to bring awareness back to the body without overwhelming it
- Practice breathwork: even gentle, extended exhales can shift your autonomic state
- Use grounding practices that engage the senses to anchor you in the present moment
This is sometimes called working within the "window of tolerance" : staying close enough to sensation to build awareness, without tipping into overwhelm.
Trauma-Informed Therapy Modalities
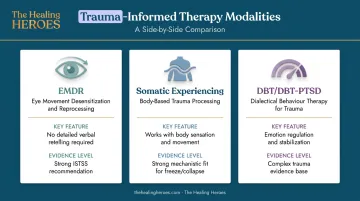
Several therapy approaches have meaningful evidence for shutdown and dissociation specifically:
- EMDR (Eye Movement Desensitization and Reprocessing): The International Society for Traumatic Stress Studies (ISTSS) gives EMDR a strong recommendation for adult PTSD. Importantly, EMDR doesn't require detailed verbal retelling of trauma in the same way as traditional exposure-based approaches , making it particularly accessible for those in shutdown states. For women with significant dissociation, stabilization work typically precedes reprocessing.
- Somatic Experiencing (SE): Developed by Peter Levine, SE uses interoception and proprioception (inner body sensation and movement awareness) to work directly with stuck defensive activation in the body. Research suggests PTSD symptom reductions, with a smaller evidence base than EMDR but strong mechanistic fit for freeze and collapse presentations.
- DBT and DBT-PTSD: For women with chronic dissociation and complex trauma, DBT provides emotion regulation and stabilization support. DBT-PTSD has shown reductions in trauma-related and dissociative symptoms in complex trauma settings.
The therapeutic relationship itself is part of what heals shutdown. A safe, attuned connection with a therapist gives the nervous system real-time experience of being seen without being harmed.
Holistic and Integrative Approaches
Yoga, mindfulness, breathwork, and acupuncture each offer meaningful support for nervous system regulation. A meta-analytic review found meditation and yoga to be promising complementary approaches for PTSD, and acupuncture research shows encouraging, if not yet definitive, results for PTSD-related symptoms.
These approaches work best alongside trauma-focused care, not instead of it. The Healing Heroes podcast has featured expert conversations across somatic healing, breathwork, EMDR, and integrative practices — a useful starting point for understanding which approaches might resonate before committing to a single path.
The Role of Safe Connection
Research consistently identifies social support as one of the most protective factors in trauma recovery. Safe relationship (whether through therapy, peer support, or trusted people who can offer presence without pressure) is not a supplement to healing. For many women, it is the mechanism through which healing happens.
When to Seek Professional Support
Some signals that professional support is warranted:
- Shutdown is interfering with daily functioning, relationships, or work
- It has been your baseline for weeks or months
- You're turning to substances, self-harm, or compulsive behaviors to "feel something" or go more numb
- You can recognize the pattern clearly but cannot shift it on your own
Finding the right fit matters. Not every modality or practitioner will feel right, and that's your nervous system giving you useful information about safety. Trust what feels right, and try a different approach if the first one feels retraumatizing.
Reaching out for help is how your nervous system finally gets what it has been missing — consistent, regulated safety with another person. That's where something new becomes possible.
Frequently Asked Questions
What is the emotional shutdown response to trauma?
Emotional shutdown is the nervous system's freeze or collapse response: an automatic protective mechanism that activates when fight-or-flight isn't possible. It involves reduced heart rate, shallow breathing, dissociation, and emotional flatness. It's an involuntary survival response, not a character flaw or a choice.
What causes people to shut down emotionally?
The primary causes include trauma (especially relational and developmental), prolonged stress, grief, and repeated experiences of emotional dismissal. Each of these overwhelms the nervous system to the point where protection feels like the only available option.
How long can an emotional shutdown last?
Duration ranges widely, from hours following a specific trigger to months or years for those with chronic or developmental trauma. Acute stress responses typically resolve within a month. Longer-lasting shutdown is a clear signal to seek professional support.
Can emotional shutdown cause physical symptoms?
Yes. Shutdown shows up physically: shallow breathing, heaviness or limpness in the limbs, reduced facial expression, slowed heart rate, and a disconnected or "out of body" feeling. These are physical signs of the nervous system's collapse response, not imagined symptoms.
Is emotional shutdown the same as depression?
They overlap but are distinct. Depression is a mood disorder; emotional shutdown is a nervous system state rooted in trauma that can coexist with depression but also occurs independently. Because the underlying mechanisms differ, treatment approaches often differ as well.
How do you help yourself come out of emotional shutdown?
Gentle body-based practices (noticing physical sensations, slow movement, extended exhales) can begin to shift the state. Connection with a safe person matters enormously. Trauma-informed professional support addresses the deeper pattern. The goal throughout is creating safety, not forcing feeling.